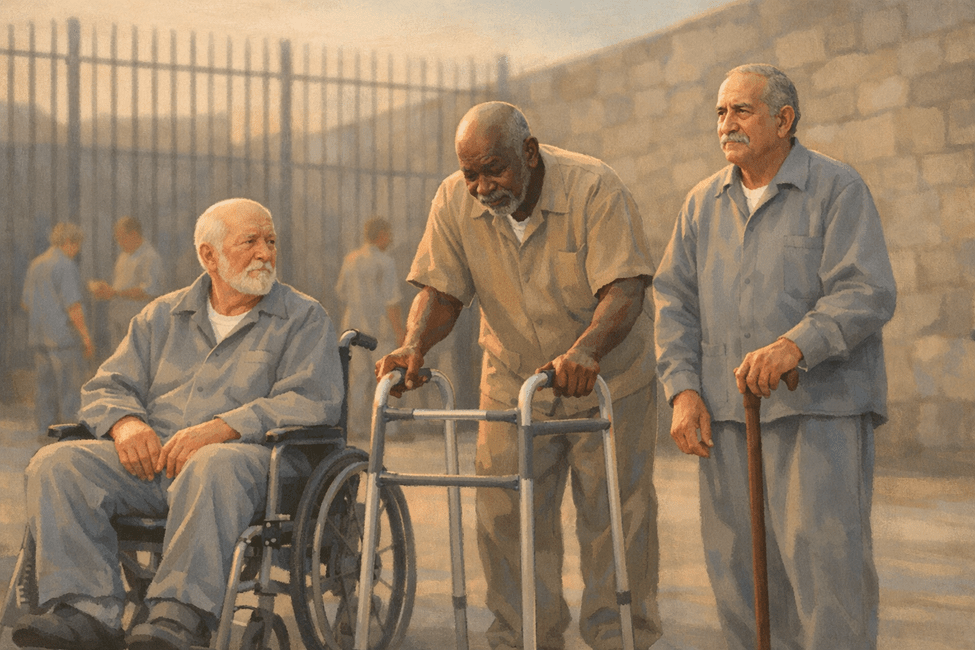
While in prison I met a lot of men that required assistance in the form of wheelchairs, walkers or canes to get around. Most of these had chronic, debilitating conditions requiring daily trips to medical to receive restricted medications and frequent offsite medical appointments. Life behind bars is tough and there isn’t any sympathy or relief from the extra challenges of getting around in a large prison compound. Come rain or shine med line callouts meant waiting outside in long lines to receive medications. Wheelchair bound inmates were assigned a wheelchair pusher to assist them with getting to appointments and meals. (Whether they showed up to do their jobs is another story.) Those with walkers or canes were on their own.
Going out of the facility for transfers or medical appointment meant belly chains and wrist & leg shackles regardless of whether you might be considered a flight risk. I had to go to the prison hospital in Jackson several times for doctor’s appointments and witnessed first-hand the pain and suffering that the sickest, frailest inmates endured to receive health care. In many ways I was blessed and fortunate to avoid illness or injury that resulted in permanent disability. For some it was a never-ending nightmare. In prison inmates have no control of their situation, and access to medical services doesn’t guarantee treatment.
I knew several inmates who had suffered medical emergencies like strokes or heart attacks. Some I knew had received traumatic injuries in fights or sports. One guy I met was suffering from liver failure and after completing his sentence with the MDOC was being held on a detainer from another state. He was looking forward to going to Ohio because there he would be eligible for a liver transplant. Prisoners in the MDOC are not allowed on the waiting lists for organ transplants. Most of the handicapped inmates I knew didn’t arrive in prison that way. I have watched a bunkie go from being an able-bodied lifer working in the kitchen to being wheelchair bound in a matter of weeks because of a change of medication ordered, not by his doctor but by a bureaucrat because there was a cheaper but less effective COPD medication available. Having life threatening conditions may not necessarily mean that you will receive treatment or that it might be changed to a lower cost, less effective treatment with devastating effects.
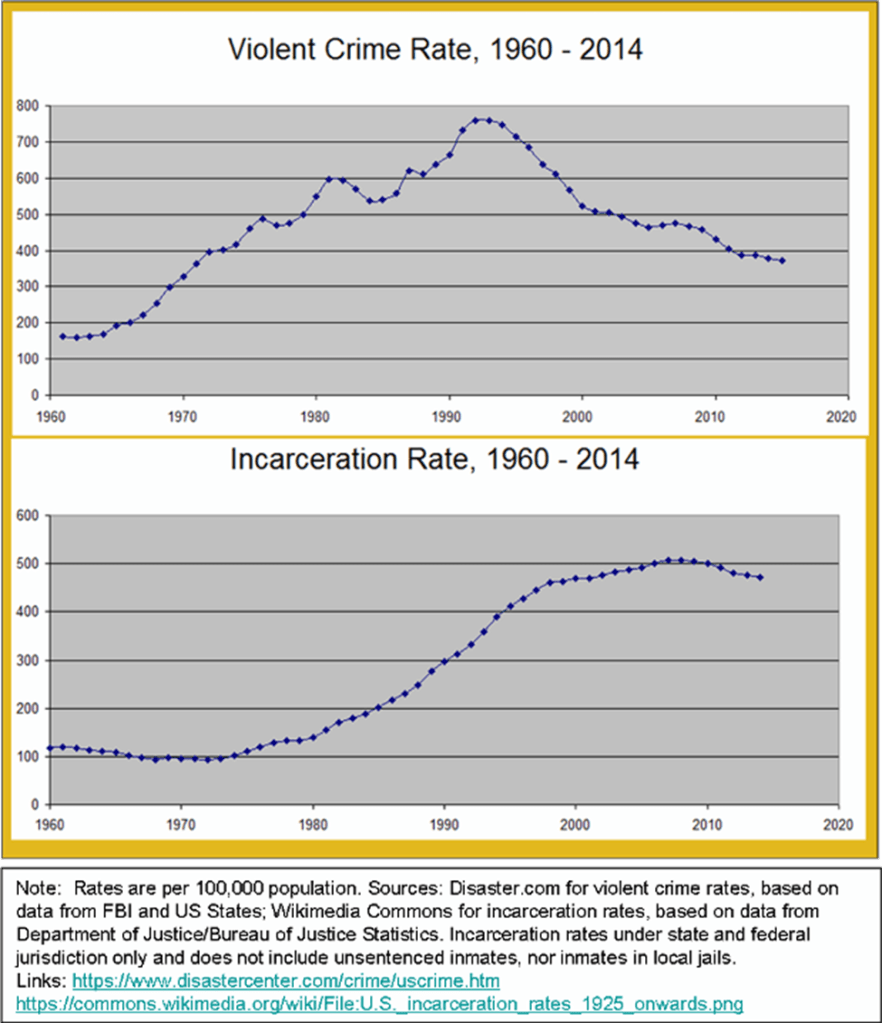
Much of how prisons operate today is based on systems developed over 100 years. Change is always slow in coming to large systems designed around a single concept- Inmates are in prison in order to “protect” the public. Prison sentences have grown longer in the last 50 years in response to public outcries and political rhetoric. Social and medical science have had little impact on these often secretive and deliberately cruel institutions. Lawsuits have had more impact on changes in prison policy and procedure than enlightened public opinion or governmental policy. “Tough on crime” legislation increased sentence guidelines and in very few cases have they been reduced, regardless of the nearly universal agreement of researchers that it hasn’t achieved the desire effect. That the human and financial costs to society are far higher than the return on investment.
Going to jail and prison are very stressful events. In my mid 40’s when I was arrested, I did not have gray hair. By the time I completed my sentence in my early 50’s my hair was turning gray. Incarceration means more than just losing your freedom, it is a complete loss of control. You no longer have a say about what happens to you. Isolation, confinement, poor nutrition, sleep deprivation, and violence all play a role in breaking you down mentally, physically and spiritually, Hours turn into days. Days turn into months. Months turn into years. Everything you once had is lost. The present is dark and scary. The future is so far away that it is unknowable. In Prison time moves slowly but inmates age faster than on the outside.
While in prison I walked the track, even ran and worked out in the weight pit some. There were sport leagues for softball, basketball and volleyball. We got out of our cells and cubes as often as we could to get fresh air and exercise. I read books from the library in order to allow my mind to visit far away places, study new ideas or work on my self improvement and spirituality. I looked forward to weekly calls home and wrote letters and created my own greeting cards. I participated in any available programming offered that I thought would look good to the parole board. But while all those things did help with the daily stresses of life behind bars, it wasn’t enough.
Prison food is legendarily awful. Most people lose a lot of weight while in jail and prison because of the inadequate portions and poor nutritional quality. Supplementing caloric intake from the store is expensive and the options are not healthy, mostly carbs and sugar. While I was at Mid-Michigan Correctional in St. Louis, MI, I even had to contend with polluted drinking water. Reports of cancers, kidney failure and other health issues that did not exist in individuals before going there have been reported, due to exposure to contaminated well water that the prison used. There have been lawsuits brought against the MDOC for food and water, but there has been little if any positive change.
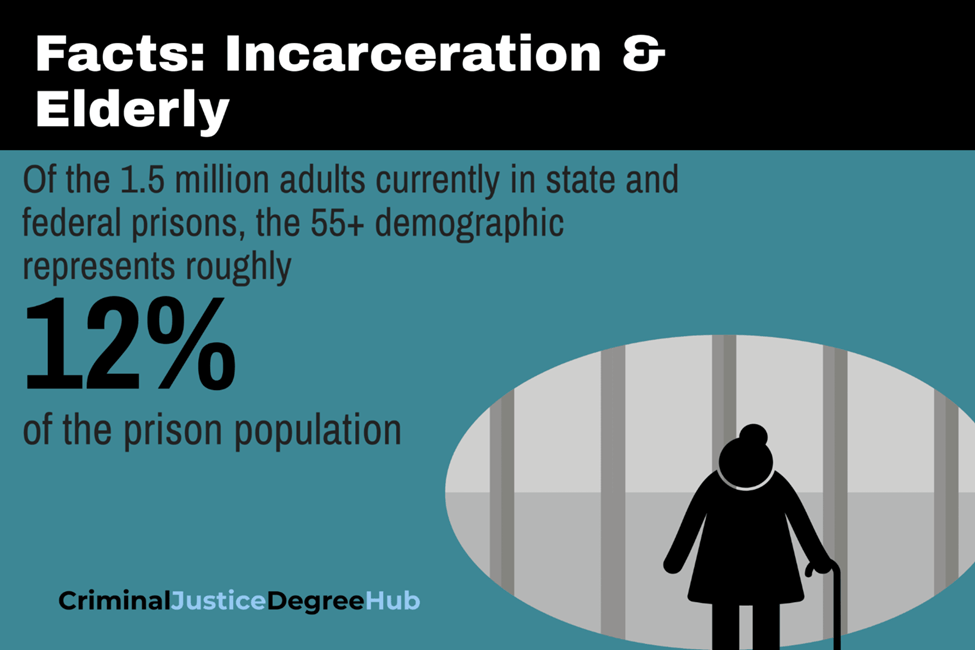
That being said there are a few items worth mentioning regarding legislative changes both recent and proposed here in Michigan, that are reflective of the conclusions drawn by researchers both in the US and internationally regarding the effects that incarceration has on individuals serving time. With the help of AI I have compiled the following overview regarding the effect that prison has on the aging of those incarcerated. To put this in context. Prison populations in Michigan and across the nation have risen dramatically since the 1980s because of longer prison sentences that legislatures enacted. Now many of those incarcerated are serving indeterminate sentences that we refer to as basketball scores. Sentences that amount to life without the possibility of parole by another name.
Accelerated Aging in Prison: Michigan in National and International Context
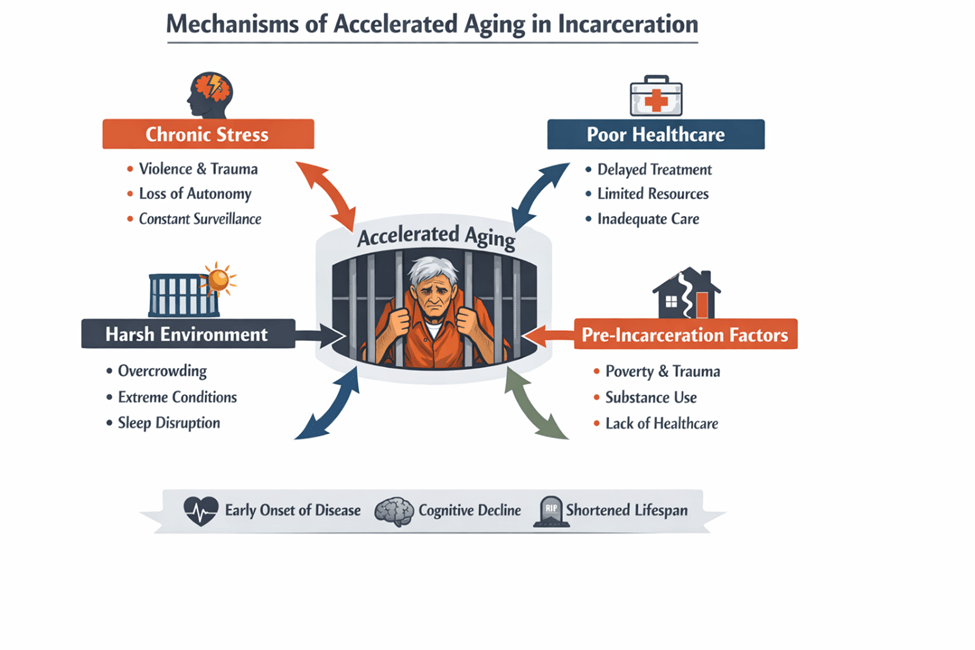
A substantial body of medical, gerontological, and social science research demonstrates that incarceration is associated with accelerated aging. Each year spent incarcerated is associated with an estimated two‑year reduction in life expectancy. Incarcerated individuals experience earlier onset of chronic disease, functional impairment, cognitive decline, and reduced life expectancy compared to the general population. As a result, people in prison are often considered physiologically 10–15 years older than their chronological age. ¹ ²
This phenomenon has direct relevance for Michigan, where a growing share of the prison population is older and medically complex, and where recent policy reforms acknowledge—though only partially address—the implications of aging behind bars.
Health and Aging in Prison
Across U.S. and international studies, incarcerated adults show:
- Earlier onset of geriatric conditions, including mobility limitations, sensory impairment, incontinence, and cognitive decline. ³
- High levels of multimorbidity at younger ages than seen in the general population. ⁴
- Elevated mortality risk and reduced life expectancy associated with time spent incarcerated. ⁵
Researchers consistently identify several drivers: cumulative life-course disadvantage prior to incarceration; chronic stress, deprivation, and loss of autonomy during imprisonment; delayed or inadequate healthcare; and prison environments designed for younger, able-bodied populations. ² ³
Michigan’s Policy Response
Michigan has explicitly recognized the challenges posed by an aging prison population and has enacted limited reforms.
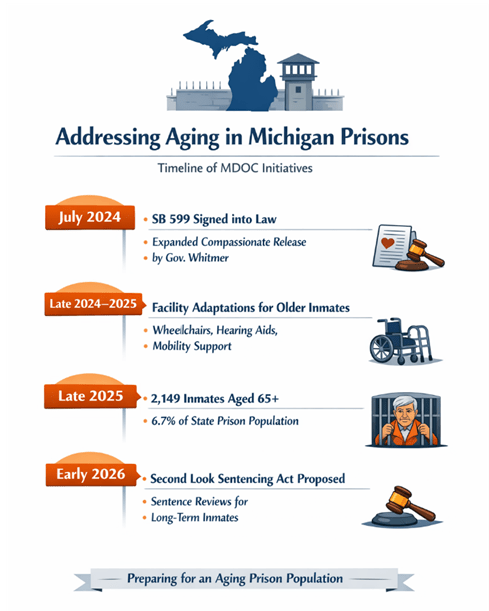
Medically Frail Parole (Senate Bill 599, Public Act 111 of 2024):
- Expanded eligibility for parole is based on serious medical conditions, terminal illness, or severe functional impairment.
- Permits release to any parole-board–approved placement, including private homes or hospice care, rather than only licensed medical facilities.
- Retains restrictive criteria focused on medical severity, low assessed risk, and minimal threat to public safety. ⁶ ⁷
Proposed Second Look Sentencing:
- Would allow judicial review of long sentences after substantial time served.
- Remains under consideration and has not yet been enacted. ⁸
Assessment:
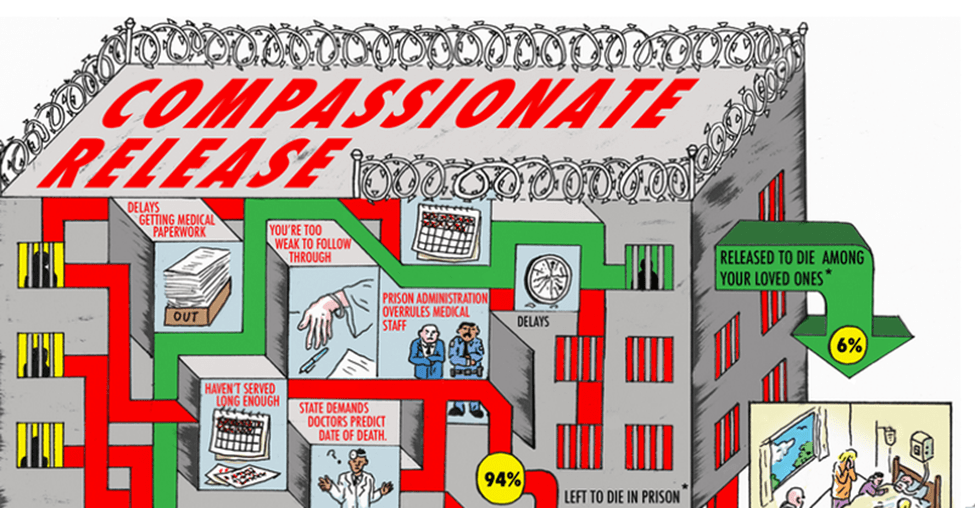
Michigan’s approach reflects a narrow, medicalized model. While SB 599 improves access to compassionate release for the most seriously ill individuals, the state largely continues to manage aging inside prison rather than broadly reassessing long sentences for older adults. I knew several inmates who tried to apply for compassionate release due to the diagnosis of terminal diseases. Only one received his compassionate release, but still died in prison before he could be released.
Comparison with Other U.S. States
State approaches to aging in prison vary considerably:
- More expansive models (e.g., California, New York):
- Provide “elder parole” or age-plus–time-served eligibility.
- Do not require terminal illness or profound disability. ⁹ ¹⁰
- Restrictive models (including Michigan historically):
- Rely primarily on medical or compassionate release with narrow eligibility and low utilization. ⁷
Michigan’s position:
Recent reforms move Michigan away from the most restrictive end of the spectrum, but it remains closer to “medically frail only” systems than to states that treat advanced age and lengthy incarceration itself as grounds for sentence review. One issue that I am aware of is that while there is a process in place to make the determination of whether or not compassionate release is warranted there was no timeframe required to make the determination, which allows MDOC staff responsible for making the determination to sit on the paperwork until it becomes a moot point.
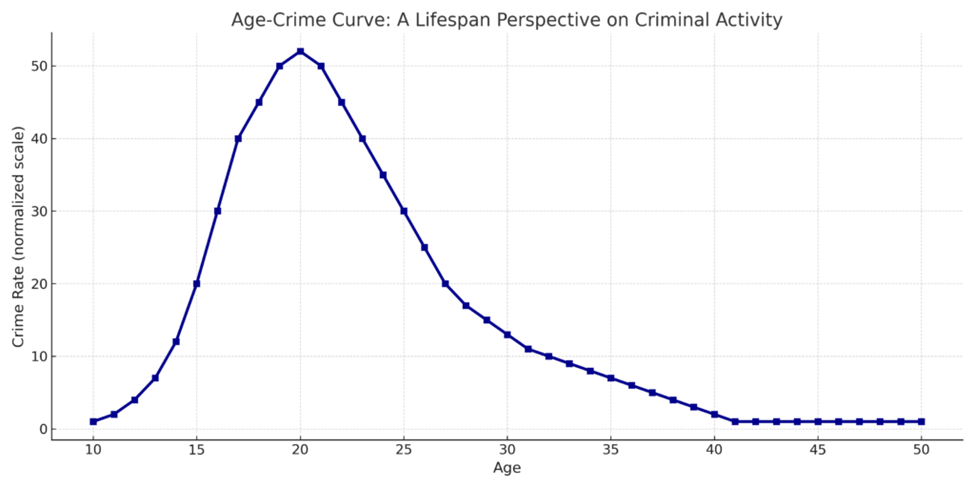
Michigan does not have “good time” or any other behavior-based system to shorten sentences to less than the Earliest Release Date. Therefore, it is not possible to go before the parole board for consideration of mitigating factors that could be taken into account in determining whether an inmate would pose a risk if paroled back into the community. Much has been said about “aging out of crime” research that shows that as people age, they tend to take fewer risks and are less likely to commit crimes in their 30s than when they were in their teens or 20s. So, for those that received long sentences based on sentencing guidelines may actually become less of a threat to society as they mature. This was acknowledged in the “juvenile life without possibility of parole” controversy where courts were ordered to resentance juvenile lifers taking their prison records into account.
Prison is a dangerous place and being older can make an inmate a target for theft, exploitation, extortion and violence. This can be especially true for older or handicapped inmates serving time for sex offenses. Sex offenders are seen as the lowest of the low and are singled out for abuse for no other reason. While sex offenses are by definition violent crimes, that doesn’t mean that the perpetrator is a violent person capable of defending themselves from gang members. Most inmates are in General Population where both violent and non-violent offenders are housed together. It isn’t possible to segregate inmate populations based on which ones are serious about going home and those that are only there on “vacation.” The violence in prison follows the same age related curve as in society. Having been assaulted twice I know how that can affect a person. Prison is no place for the weak and defenseless but there are too many there that are just that. People to weak to pose a threat to society but are unable to be considered for any type of “unfitness for prison” designation as some other countries have.
International Comparison (United Kingdom and Europe)
International research and policy frameworks generally adopt a different orientation:
- Aging in prison is framed primarily as a human rights and dignity issue, not solely a healthcare problem. ¹¹
- Release decisions often focus on whether continued detention is compatible with frailty, severe disability, or cognitive impairment, rather than on diagnosis alone. ¹²
- Greater reliance on shorter sentences, non-custodial sanctions, and compassionate release reduces the number of people aging in custody. ¹¹
- Universal or integrated healthcare systems facilitate continuity of care following release. ¹³
Compared with these models, Michigan—like most U.S. states—places greater emphasis on managing aging within prison rather than structurally limiting long-term incarceration of older adults.
Comparative Approaches to Aging and Release from Prison
| Dimension | Michigan (MDOC & State Law) | Other U.S. States | International Models (UK / Europe) |
| Primary mechanism for older or infirm prisoners | Medically frail parole under SB 599 (Public Act 111 of 2024); proposed but unenacted Second Look Sentencing¹² | Mix of medical parole, geriatric/elder parole, resentencing, and executive clemency; scope varies widely by state³⁴ | Compassionate or medical release combined with generally shorter sentences and broader use of non‑custodial sanctions⁵⁶ |
| Trigger for release | Serious or terminal medical condition, severe functional impairment, dementia, minimal public‑safety risk¹ | Often age plus time served (e.g., 50–65 years old with 10–25+ years served), sometimes without terminal illness requirement³⁷ | Terminal illness, severe disability, or determination that continued detention is incompatible with dignity or human‑rights standards⁵⁸ |
| Placement after release | Any parole‑board–approved placement, including private homes or hospice (expanded by SB 599)¹ | Some states require placement in licensed medical facilities; others allow home or community placement³ | Typically home, hospice, or community care settings, often integrated with national health systems⁶⁹ |
| Definition of eligibility | Narrow and medicalized: diagnosis‑ and impairment‑based; age alone is insufficient¹² | Highly variable; some states recognize “geriatric” status by age, others rely almost exclusively on medical criteria³⁴ | Often framed as “unfitness for imprisonment” or disproportionate punishment, rather than age or diagnosis alone⁵⁸ |
| Overall policy orientation | Incremental and restrictive; focuses on releasing only the sickest individuals while most age and die in prison¹² | Patchwork system: ranges from expansive elder‑parole frameworks to rarely used medical release mechanisms³⁴ | Greater emphasis on proportionality, dignity, and limiting long‑term incarceration of frail or elderly people⁵⁶ |
Key Takeaways
- Research consensus: Prisons are aging-accelerating environments.
- Michigan: Acknowledges accelerated aging but relies on narrow, medically driven release mechanisms.
- Other U.S. states: Offer a patchwork ranging from restrictive medical parole to broader elder-parole systems.
- International models: Emphasize proportionality, dignity, and reduced reliance on incarceration for older and frail individuals.
Bottom line:
Michigan has made incremental progress but compared with more expansive U.S. reforms and international approaches, it continues to prioritize selective medical release over broader reassessment of long sentences and the appropriateness of incarcerating older adults.
The research also shows that the effects of aging in prison are not easily mitigated after parole. These are life expectancy shortening, quality of life issues that are the unintended consequences of incarceration. In a society solely focused on retribution rather than rehabilitation and reconciliation there needs to be more discussion, not based on emotions but rather on scientific evidence to guide decision making. There needs to be less of a proscribed one-size-fits-all approach to sentencing guidelines and more of an individual evaluation of whether or not a person is still considered a threat to society. Give the parole and clemency boards the ability to determine if the time spent in prison has resulted in meaningful and measurable reform. Provide more structural support during parole to ensure the successful reintegration back into society. All of these things together would reduce prison populations and minimize this aging effect, thereby reducing long term costs associated with incarceration and medical care.
Footnotes
- Berg, M. T. et al., Losing Years Doing Time: Incarceration Exposure and Accelerated Biological Aging, Journal of Health and Social Behavior (2021).
- Doherty, E. E. et al., Examining the Relationship Between Incarceration and Healthy Aging, Journal of Developmental and Life‑Course Criminology (2025).
- Prison Policy Initiative, Graying Prisons: States Face Challenges of an Aging Inmate Population (2018).
- American College of Physicians, Health Care Implications of the Rapidly Aging Incarcerated Population.
- ACLU & Prison and Jail Innovation Lab, Trapped in Time: The Silent Crisis of Elderly Incarceration (2025).
- Michigan Legislature, Senate Bill 599 (Public Act 111 of 2024).
- Michigan Allows More Releases for Medically Frail Prisoners, Prison Legal News (2025).
- WCMU Public Media, reporting on proposed Second Look Sentencing legislation.
- National Conference of State Legislatures, analysis of elder parole statutes (cited in The Marshall Project, 2026).
- Davis Vanguard, Debate Grows Over Elder Parole Bill in New York (2026).
- Prison Reform Trust, Growing Old in Prison (UK).
- UN Office of the High Commissioner for Human Rights, submissions on older persons deprived of liberty.
- Gavin, P. et al., Healthcare and Social Care Needs of Older Prisoners in England and Wales, Social Sciences (2025).
Table Footnotes
- Michigan Legislature, Senate Bill 599 (Public Act 111 of 2024), amending medically frail parole eligibility.
- Michigan Allows More Releases for Medically Frail Prisoners, Prison Legal News (2025).
- National Conference of State Legislatures, surveys of elder‑parole and geriatric‑release statutes (cited in The Marshall Project, 2026).
- How States Are Grappling With an Aging Prison Population, The Marshall Project (2026).
- Prison Reform Trust, Growing Old in Prison (UK).
- Gavin et al., Healthcare and Social Care Needs of Older Prisoners in England and Wales, Social Sciences (2025).
- Davis Vanguard, Debate Grows Over Elder Parole Bill in New York (2026).
- UN Office of the High Commissioner for Human Rights, submissions on older persons deprived of liberty and compatibility of detention with human‑rights standards.
- Penal Reform International, Global Prison Trends and European prison‑health integration analyses.
