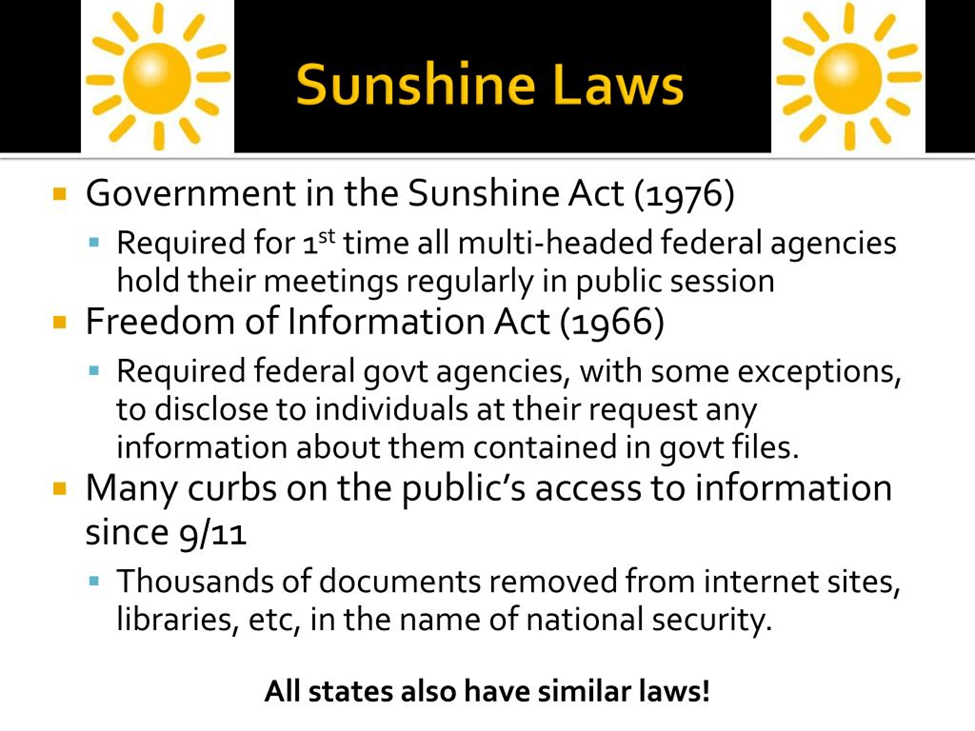
May is Unlock the Box Mental Health Awareness Month. The Unlock the Box Campaign is a coalition of organizations and movement leaders who partner with state and local campaigns across the United States with the common goal of ending the use of solitary confinement for all people. Currently active in 22 states and the District of Columbia, including Michigan. Open MI Door is the organization leading the fight in Michigan. OMD is seeking to affect policies and practices in all Michigan prisons, jails, and juvenile facilities. Current focus is on ensuring transparency, accountability, and independent oversight in the use of isolation and in conditions of confinement in general.
The statistics regarding the effects of solitary confinement are alarming. Right now, there are at least 122,000 people being held in solitary confinement in the United States. Over a third of people subjected to solitary confinement become psychotic and/or suicidal within the first 15 days. Individuals who have been in solitary confinement are 78% more likely to commit suicide within a year of their release from prison.
The Michigan Department of Corrections, or MDOC, does not usually use the phrase “solitary confinement” in its internal rules. Instead, it describes the practice as “segregation” or “restrictive housing.” That language matters, because bureaucratic terms can make an extreme practice sound routine. But the reality described in the department’s own policy materials and in the references collected here is unmistakable: segregation means isolating people from the general prison population, often for 23 to 24 hours a day, with sharply restricted movement, limited human contact, and minimal access to ordinary programming. MDOC policy presents segregation as a management tool used for discipline, control, and protection, while critics argue that it functions as a deeply harmful form of isolation that causes lasting psychological damage and undermines rehabilitation.

Michigan’s system illustrates the central contradiction in the national debate over solitary confinement. Prison administrators defend segregation as necessary in some cases to manage violence, serious misconduct, escape risk, or threats to vulnerable prisoners. At the same time, decades of reporting, advocacy, and international human-rights standards have increasingly challenged prolonged isolation as unsafe, inequitable, and incompatible with basic human dignity. Even MDOC’s own reporting shows that the department has sharply reduced administrative segregation over time, suggesting that the state itself recognizes that heavy reliance on this practice is neither inevitable nor desirable. The question is no longer whether segregation is severe. The question is whether Michigan should continue to rely on it in its current form. The strongest answer, based on the material in this document and the cited sources, is no: prolonged segregation should be discontinued and replaced with tightly limited, reviewable, therapeutic, and safety-focused alternatives.
What Segregation Means in the MDOC
According to MDOC policy, segregation is not a single category but a system with several forms. Temporary segregation is short-term isolation used while staff investigate alleged misconduct or await a hearing. Punitive segregation is imposed as a disciplinary sanction after a person is found guilty of a major misconduct violation. Administrative segregation is the most troubling category because it can become long-term. It is reserved for people that the department considers serious threats to institutional safety, major escape risks, unmanageable in general population, or in need of protective separation. On paper, each category has a different purpose. In practice, all three involve versions of extreme separation from ordinary prison life.
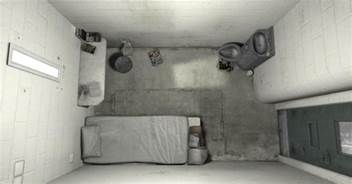
The living conditions are severe. People in long-term segregation may spend nearly the entire day alone in a cell of roughly 70 to 80 square feet. Human interaction is drastically limited. When they leave the cell, they may be shackled. Exercise is restricted and often takes place in enclosed spaces rather than meaningful recreation areas. Meals are delivered through a slot in the door. Showers and other basic activities are tightly controlled. These are not incidental inconveniences. They are the core features of an environment built around deprivation, surveillance, and social isolation.

MDOC also emphasizes that segregation is regulated through reviews. Placement decisions are supposed to be examined by a housing unit team, the Security Classification Committee, wardens, and in longer cases higher-level administrators. Those review requirements are important, but they do not erase the underlying harm of isolation. The system can be procedurally structured and still be substantively damaging. If the practical result is that a person spends months or years in near-total isolation, repeated reviews do not change the nature of the confinement. They only document it.
Why MDOC Uses Segregation
MDOC’s own policy language makes its rationale clear. Segregation is used, in the department’s words, to achieve effective administrative management, maximum disciplinary control, and individual prisoner protection. That means the practice is justified on three main grounds. First, it is used as punishment for major misconduct. Second, it is used as a security tool when officials believe someone presents a danger to staff or other incarcerated people. Third, it is used, at least sometimes, to separate people who may themselves be at risk of harm in the general population.
Those reasons are not frivolous. Prisons are coercive environments, and correctional administrators are responsible for preventing violence and responding to emergencies. There are situations in which immediate separation is necessary. A person who has just committed a serious assault, threatened staff, or faces a credible risk of being attacked may need to be removed quickly from the general population. Any honest analysis should acknowledge that reality. The problem is that a short-term emergency separation tool is not the same thing as a long-term isolation regime. What may be justified for hours or days becomes far harder to justify when it stretches into weeks, months, or years.
Michigan’s own recent policy developments suggest that the state understands this distinction. The department has reported large reductions in segregation since 2008 and has developed Structured Alternative to Administrative Segregation (START) units as alternatives for some prisoners with serious mental illness. Those reforms implicitly recognize that segregation has often been overused and that at least some of the people once held there can be managed differently. If safer alternatives exist for many cases, then prolonged segregation is less a necessity than a policy choice.
What the Outcomes Show
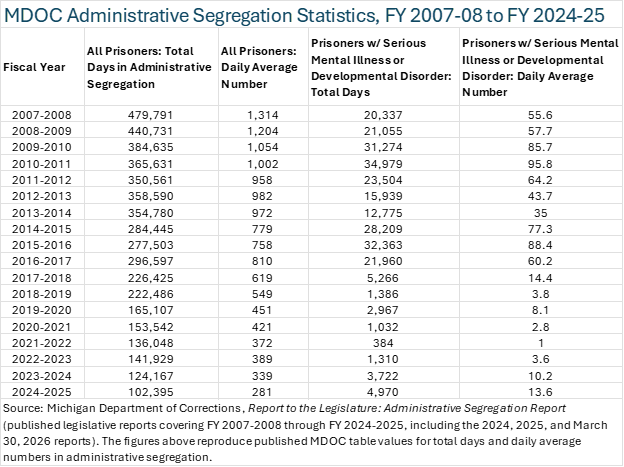
One of the clearest outcomes in the record is that Michigan has reduced its use of administrative segregation substantially. The data table shows a decline from 479,791 total segregation days and a daily average population of 1,314 in fiscal year 2007–2008 to 102,395 days and a daily average of 281 in 2024–2025. That is a dramatic drop. It undermines any claim that Michigan must rely on segregation at the levels it once did. If the prison system can function with far fewer people in administrative segregation than it held there in 2008, then the older level of use was not an unavoidable feature of prison management. It was an institutional practice that could be changed.
At the same time, a reduction in volume does not resolve the moral and practical concerns. Hundreds of people are still held in administrative segregation, and some remain there for periods exceeding 3, 6, or 12 months. That matters because the harms of segregation are not measured only by how many people are isolated, but also by how long the isolation lasts. The United Nations Nelson Mandela Rules define solitary confinement as confinement for 22 hours or more a day without meaningful human contact, define prolonged solitary confinement as anything beyond 15 consecutive days, and prohibit indefinite and prolonged solitary confinement as inconsistent with minimum standards for humane treatment. Michigan’s own reports showing people in segregation for months or longer place the state in direct tension with those standards.
The human outcomes described in the references are equally serious. Advocates, family reports, legal analyses, and broader research on solitary confinement consistently associate prolonged isolation with anxiety, depression, cognitive deterioration, self-harm risk, hopelessness, and worsening symptoms for people with mental illness or developmental disabilities. Even when corrections officials present segregation as a safety measure, the evidence suggests that isolation can destabilize the very people the institution is trying to manage. That creates a damaging cycle: distress leads to misconduct, misconduct leads to more isolation, and more isolation deepens distress.
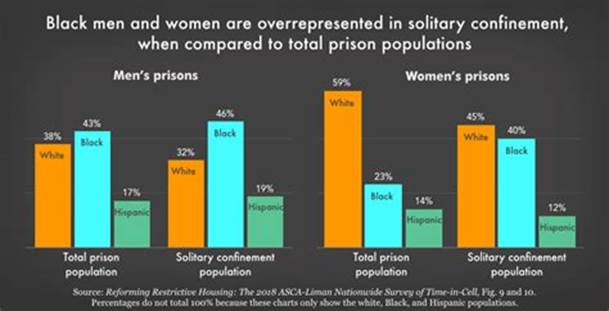
There are also broader institutional outcomes. Segregation can make reentry into the general prison population harder by eroding social functioning and increasing distrust. It can also make release into the community more dangerous when people leave prison directly from highly isolating conditions without adequate step-down support. And the practice appears to fall unevenly across the prison population. The materials in this document point to racial disparities in segregation use, with Black men overrepresented in segregated housing compared with their share of the overall prison population. That raises an additional reform concern: segregation is not only severe but may also be administered inequitably.
Additional support for ending prolonged segregation comes from the Unlock the Box campaign, a national coalition focused on abolishing solitary confinement in the United States. The campaign argues that solitary is not only harmful but also counterproductive. Its public materials describe solitary confinement as extreme isolation for 22 or more hours a day, note that an estimated 85 percent of people in solitary are there for nonviolent disciplinary reasons, and report that as many as one-half of those in solitary live with mental illness that isolation can worsen. Unlock the Box also emphasizes that prolonged solitary confinement does not make prisons or communities safer, and that people of color are disproportionately subjected to it beyond their already disproportionate representation in prison populations. Those points reinforce the case that prolonged segregation in Michigan should not be treated as an unfortunate but necessary norm; it should be understood as a policy choice with predictable harms and unequal effects that demand correction.
Segregation and Human Rights
The international human-rights case against prolonged segregation is powerful and increasingly specific. The United Nations Nelson Mandela Rules do not treat isolation as a neutral administrative option. They treat it as a practice requiring strict limits because of its potential to become cruel, inhuman, or degrading treatment. Under those rules, prolonged solitary confinement means more than 15 consecutive days, and indefinite solitary confinement is prohibited. The rules also emphasize that solitary confinement should be used only in exceptional cases, as a last resort, for the shortest possible time, and subject to independent review. They further state that it should not be used when a prisoner’s mental or physical disability would be exacerbated by the measure.
Measured against that standard, Michigan’s regime raises serious concerns. The state may call the practice administrative segregation, temporary segregation, or punitive segregation, but a change in terminology does not change the lived reality of isolation. If a person is locked down for 22 to 24 hours a day with little meaningful human contact, then the practice falls within the human-rights framework developed by the United Nations. And if that confinement continues for months, as Michigan’s own reports show happens in some cases, then the state is operating beyond the threshold the Mandela Rules identify as prolonged solitary confinement.
Some defenders of the current system argue that prison safety justifies these departures. Safety is important, but human-rights standards already account for that argument. The Mandela Rules do not forbid every temporary emergency separation. They forbid turning isolation into a routine or open-ended instrument of prison governance. That distinction is crucial. A correctional system can protect staff and prisoners while still rejecting prolonged solitary confinement. In fact, Michigan’s own reduction in segregation usage suggests that reform is compatible with institutional order. The human-rights issue is therefore not whether prison officials ever need tools for emergency separation. It is whether the state should keep using prolonged isolation after it knows the damage it causes and after alternatives have already been shown to exist.
Should Michigan Discontinue Segregation?
If the question means whether Michigan should eliminate every form of temporary emergency separation, the answer is probably no. Prisons need a narrow capacity to separate people immediately after violence, during investigations, or when a person faces an imminent threat. But if the question is whether Michigan should discontinue prolonged segregation as a standing correctional practice, the answer should be yes. Long-term isolation should end.
There are several reasons for that conclusion. First, the harms are too severe. Segregation can intensify mental distress, undermine stability, and damage the social capacities people need both inside prison and after release. Second, the practice is inconsistent with modern human-rights standards once it extends beyond very short periods. Third, the state’s own declining segregation numbers show that Michigan can reduce its use substantially without abandoning prison administration altogether. Fourth, indefinite or months-long isolation invites arbitrary and unequal outcomes, especially where racial disparities and mental health concerns are already present.
Discontinuing prolonged segregation does not mean ignoring violence or misconduct. It means replacing a blunt and damaging tool with more precise responses: short emergency separation, intensive mental-health intervention, structured step-down units, restorative or behavior-based programming, and individualized safety planning for those who need protection. A prison system committed to safety should prefer methods that reduce future harm rather than deepen it.
What Reform Should Look Like
Real reform in Michigan should begin with a clear legal time limit that brings state practice closer to the Mandela Rules. The legislature should prohibit prolonged solitary confinement, ban indefinite segregation, and require meaningful out-of-cell time, programming, and regular independent review for anyone held apart from the general population. People with serious mental illness, developmental disabilities, and other especially vulnerable conditions should not be placed in isolating units that predictably worsen their condition.
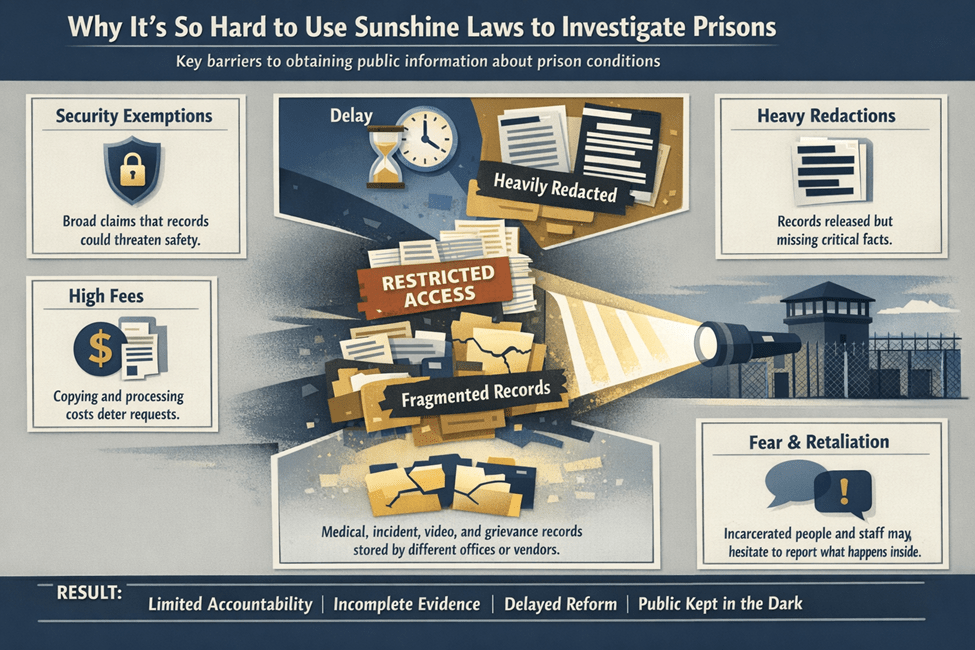
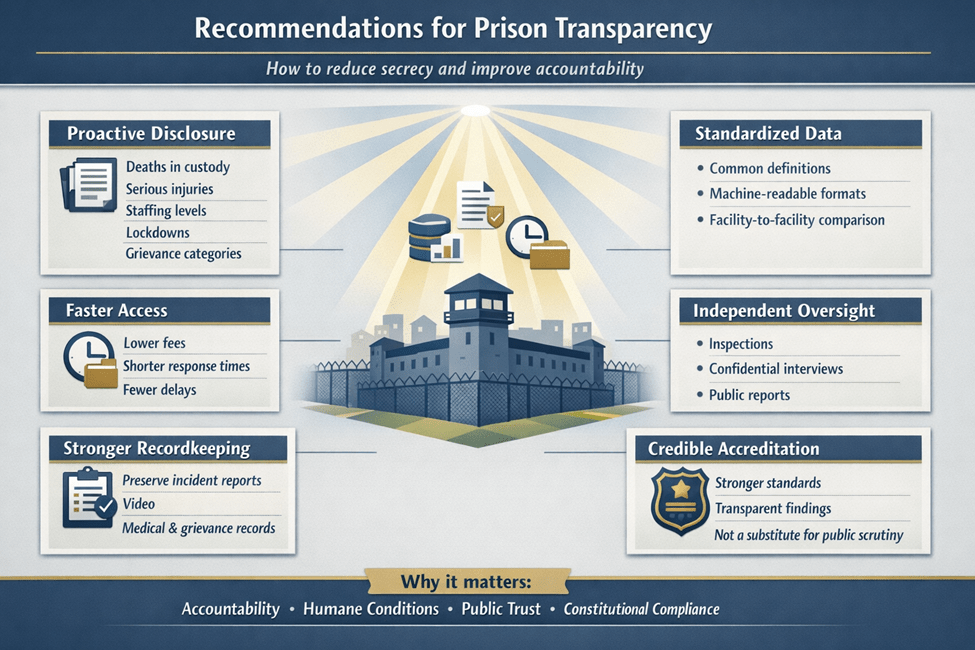
Reform should also require transparency. Michigan already reports some segregation data, but durable accountability needs more than aggregate totals. Public reporting should include duration, facility-level usage, demographic patterns, mental-health status, reasons for placement, and release pathways from segregation. The point of transparency is not only to monitor numbers; it is to expose whether the system is relying on isolation as a substitute for staffing, treatment, training, or conflict resolution.
Finally, reform must include culture change. Segregation survives not only because policies authorize it, but because institutions become accustomed to treating isolation as normal. That habit is hard to break. Michigan should invest in staff training, behavioral de-escalation, therapeutic housing, and transition units that prepare people to return safely to prison programming and eventually to the community. If the state is serious about rehabilitation, it cannot continue to rely on a practice that strips people of meaningful human contact and then expects them to emerge healthier, safer, or more prepared for life after incarceration.
Unlock the Box also helps clarify what reform can look like in practice. Its campaign materials highlight legislative approaches that prohibit solitary confinement beyond 15 days in line with the Mandela Rules, create independent oversight, protect vulnerable groups, and in some proposals reduce isolation for emergency de-escalation to only a few hours while requiring safe and humane alternatives. That framework supports a practical reform agenda for Michigan: narrow the grounds for separation, impose strict time caps, expand therapeutic and program-rich alternatives, increase meaningful out-of-cell time, and ensure that any temporary separation is genuinely brief and tied to a clear transition plan back to less restrictive conditions.
Segregation in the Michigan Department of Corrections was built on the idea that isolation can produce order. The evidence suggests something more complicated and more troubling: isolation may sometimes create temporary control, but it does so at high human cost and with serious legal and moral consequences. Michigan has already shown that it can reduce segregation. The next step is to go further by ending prolonged isolation, preserving only tightly limited emergency separation, and building a correctional system centered on safety, treatment, accountability, and human dignity.
Open MI Door is fighting for the passage of bill SB493, which seeks to expand the powers and duties of the Legislative Corrective Ombudsperson’s Office as a meaningful step forward in bringing our state into full compliance with the UN’s Mandela Rules. If you know someone in prison or who has been in prison check out the mental health resources available on the OMD website.
References
Michigan Department of Corrections. Policy Directive 04.05.120: Segregation Standards. Effective June 1, 2019.
Michigan Department of Corrections. Report to the Legislature: Administrative Segregation Report. March 30, 2026.
United Nations General Assembly. United Nations Standard Minimum Rules for the Treatment of Prisoners (the Nelson Mandela Rules), A/RES/70/175. January 8, 2016.
U.S. Department of Justice. Report and Recommendations Concerning the Use of Restrictive Housing. January 2016.
Luigi, M., Dellazizzo, L., Giguère, C.-É., Goulet, M.-H., & Dumais, A. “Shedding Light on ‘the Hole’: A Systematic Review and Meta-Analysis on Adverse Psychological Effects and Mortality Following Solitary Confinement in Correctional Settings.” Frontiers in Psychiatry, 11 (2020).
Vera Institute of Justice. The Impacts of Solitary Confinement. April 2021.
Unlock the Box Campaign. About Us; Resources: Solitary by the Numbers; and Experience. Accessed May 16, 2026.